Lately I have become part octopus, part mountain goat and part fish.
The octopus part of me has been juggling tasks at work like crazy. I spent the last couple of months organizing a big festival while also having a bunch of other programs to design and lead. One weekend I was teaching a nature-sketching workshop, the next a toddler class on toads. When I am done typing this post I need to practice my guitar for an upcoming campfire program. I have longed to come home and do something relaxing after this whirlwind, but that is not in the cards this summer. What is on the agenda is Rainier and I need to use every spare minute getting my body ready for the climb.
This leads me to my mountain goat side. Just about every weekend, Doug, his dad and I have climbed a 13,000- or 14,000-foot peak. Each time we do one of the hikes, we have been increasing the weight in our backpacks. Our last hike took us to 14,141-foot South Mt. Elbert. The hike was around 10 miles round trip and I was able to carry 45 pounds with 4,500 feet of elevation gain. I felt really strong and was ecstatic with the accomplishment because this is similar to what I will have to do on Rainier. I still have just over a month of training time before the trip so the plan is to keep doing hikes of this nature, including a few overnight trips, so that we can begin to move more quickly and efficiently on steep terrain with heavy packs. Some evenings after work I have also been going up to the Flatirons in Boulder, CO to hike some shorter and lower (though still steep) peaks.




So far, my joints have been doing great through my training regime. Part of this has to do with the comprehensive physical therapy program I am on. Between my shoulder, hip and Achilles exercises, I spend about 45 minutes most days on physical therapy. It taxes my schedule and makes me stay up later on some nights than I would like, but the benefits have been huge.
The other reason I think that my joints have been doing so well is that I discovered a new exercise: deep-water running. Hiking one or two big peaks each week with a heavy pack is hard on my joints, so in between I have decided to skip running, climbing, zumba and even biking to train as these all make my Achilles tendonitis flare up. I know I will return to all these activities when I get back from Rainier as my Achilles is basically already healed. However, for now I just don’t want to risk re-injuring it since things are going so well and I am able to hike long distances with elevation gain again. I had tried swimming to increase fitness, but the repetitive arm motions aggravated the avascular necrosis in my shoulder. I knew that I had to complement the long weekend hikes with something in order to get enough cardiovascular training in mid-week. But what activity?
I took to the internet to get some ideas and there I discovered the perfect training activity: deep-water running. Doing this exercise would help me build up cardiovascular fitness and muscle strength while giving my joints a chance to rest from the long hikes I was also doing. A quick Google search revealed several instructional videos on deep-water running. and it looked pretty easy. It basically involved putting on a floatation belt, going to the deep end of a pool and running almost like you would on land. The running form ends up being slightly different, but the videos provided enough guidelines that I felt confident to give it a go.
The first time I ventured to the gym to try the new activity I felt awkward because I didn’t travel very far when running in the deep end of a pool. On land, when you increase your running speed and intensity you generally travel a much greater distance. In the the pool, I can run as hard as possible and only travel 15 feet. It reminds me of crazy nightmares where I am being chased by ghosts, monsters or bandits and I am running really fast to get away but not getting anywhere. When I exhaust the length of the deep end, I turn around and head the other direction.


Running in small circles in this way doesn’t feel very interesting compared to running on a scenic trail, but I have to remind myself that it is really no different than running on a treadmill. However, the cardiovascular benefits are huge. Deep-water running really gets the heart rate up. Not to mention that the resistance the water provides has helped me build muscle–and not just in my legs. I move my arms underwater just like I do when I run on land, but because the resistance is so much greater, I have noticed my arms are getting a lot stronger too.
As on land, one has to pay attention to their running form in the water. I find that if I am getting lazy about form, I will start treading water instead of running. Treading water is not nearly as strenuous as running and does not get my heart rate up to an adequate training level. To make sure I am keeping my form, I will actually close my eyes and picture myself running on a trail or road and try to mimic that movement in the pool. Another trick that works well for me is to pick a stationary object on the edge of the pool and pretend it is another runner in a race that I am trying to catch. Both of these things help ensure that I stay in good form and keep my heart rate up.
For workouts, I usually deep-water run for about 45 minutes to an hour and then soak in the hot tub for 15 minutes which feels amazing on my joints. I have been deep-water running 2-3 times a week. A lot of people may be wondering if this influences my ostomy appliance wear-time. I find that being in the pool and hot tub this much does not affect my appliance’s ability to adhere. However, I change my appliance every three to four days regardless of what activities I do. Perhaps if someone was trying to get a seven-day wear-time, swimming might shorten it a bit.
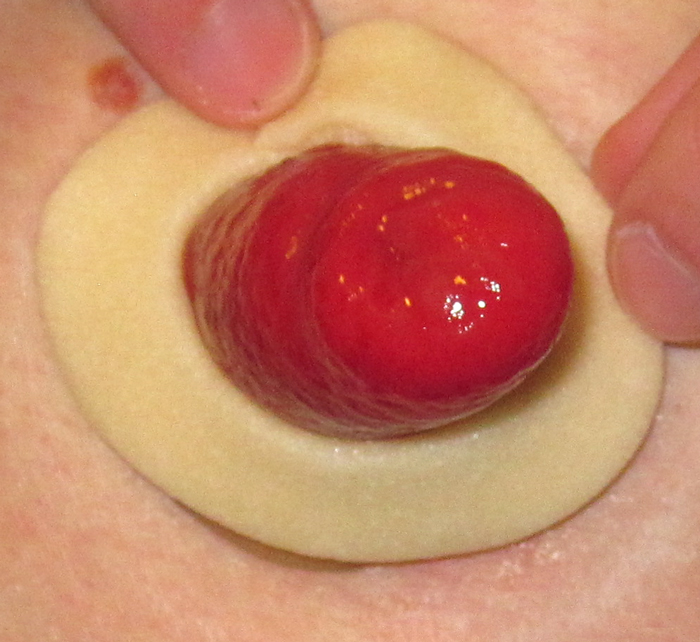
I also do not have to do anything different to get my appliance to stay on in the pool. I basically jump in with my wafer as is (my wafer method is pictured in this post). Some people who have had issues with their appliances staying on in the water have great luck with products such as Sure Seals and Coloplast Brava Elastic Barrier Strip. I have tried both and they work well. I just find that my appliance sticks fine without them for the amount of swimming I do. If I were to take a beach vacation or a trip to a water park where I was in the water all day I would definitely use these. As far as swimming attire when I am deep-water running, I wear a variety of tankini tops with swim shorts and then an Ostomy Secrets Swim Wrap which covers the part of my pouch that sticks out above the low-rise swim shorts.
If you are looking for a gentle-on-the-joints exercise to gain strength I would recommend deep-water running. I only wish I had discovered this activity sooner after surgery. It would have been a great low-impact way to get back into shape once my incision was healed and I could return to water sports.
For now, it has become this octopus-mountain goat-fish’s best option for getting in shape for Rainier. It fits into the busy work schedule, is easy on the joints, and gets the heart pumping. I am feeling more optimistic then ever that as long as the weather cooperates for our ascent, I will be strong enough to stand on that summit.